Half the service respondents described experiencing difficulties in providing carer support. Both of the independent hospitals had had problems setting up or maintaining their levels of support. Slightly more NHS units (55%) had not, compared to those that had, experienced difficulties. Several services stated that difficulties arose because carers were not interested in engaging with forensic mental health services, or that the patients in their particular service tended to be estranged from, or not in ongoing contact with their relatives, thus complicating their attempts to engage with carers. One ward which supports patients both with and without a forensic history noted that:
Current forensic carers were significantly less likely to accept support and engagement offered than their generic counterparts… only one patient’s carers had ever attended a CPA review.
There was nothing to suggest that the service had found out why take up was poor or used alternative means of engaging and supporting carers to attend review meetings. Even where services reported they had contacted eligible carers to invite them, for example, to join a support group, uptake could be so low that it did not justify the allocation of staff and resources. The reasons given for this lack of engagement were suggested to involve travel distances and suspicion of services. One respondent emphasised that there are opportunities for all staff to be more pro-active about contacting carers:
There has been times recently with new consultants who do not contact relatives when patients are admitted so families may not know where their son is etc. and that is difficult for us as nurses to deal with as it could only be a ‘your son is safe’ phone call but also a lot of useful, essential information can be gathered re: someone’s illness from such a call.
One community service reported initial difficulties with staff commitment to the carers group because of a dislike of working evenings. To counter this, the group was staffed via a rota, but this perhaps diluted continuity of staff involvement. This problem was solved by a particular member of staff finding they enjoyed the work so much that they volunteered to staff the group permanently. This speaks of the potential for staff involvement in carer support to maximise job fulfilment, but might suggest some potential service vulnerability to staff illness or turnover. It also indicates that the service did not see carer involvement as part of its core work.
One fifth of services stated that they did not systematically monitor or evaluate the support offered to carers. While not systematic, the most commonly cited mechanism used was to ‘obtain direct feedback from carers’, followed by questionnaire surveys. The State Hospital conduct an annual survey of this kind.
The average percentage of carers reported to be using support across all types of forensic mental health services was 43%, with a range from zero engagement to 100%. Particularly high estimations came from one of the State Hospital hubs, who reported 100% involvement of carers through the Visitors Centre, and respondents from low secure for learning disability services. Those estimating low uptake included all the medium secure units, one of the private units, an IPCU, a community forensic team and a day centre. Table 6 below shows that most respondents estimated uptake to be in the low to medium categories.
Table 6: Estimated percentages of carers who use support provided by forensic mental health services
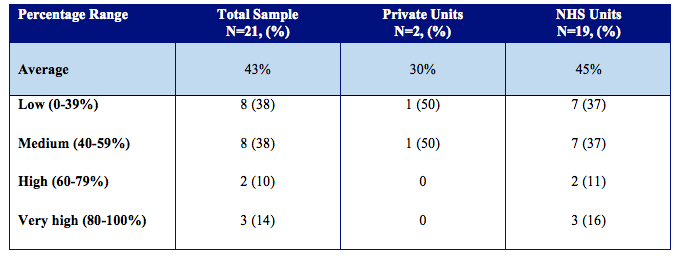
Table 7 below shows that the main reasons why staff in forensic mental health services believed that carers did not take up the available support were predominantly about carers’ own choices and circumstances, or with the stigma associated with caring for a relative in forensic mental health services. In this regard, the carer’s choice was rated as the most likely reason by four out of five of respondents, followed next by geographical challenges, and, related to this, transport, and then stigma of the forensic label. Both independent hospitals cited geography and travel as the key reasons.
Table 7: Service perceptions for low levels of carer engagement with support
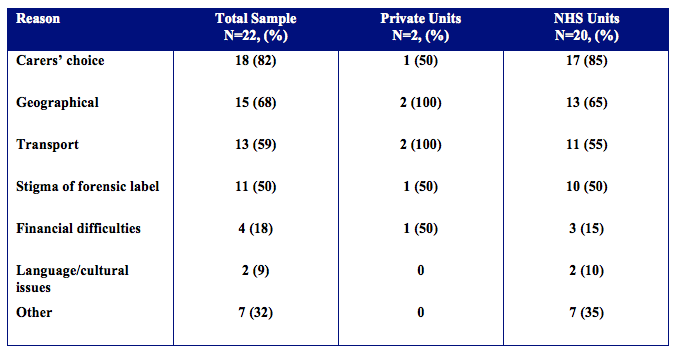
Most comments from the survey indicated that staff opinions about carers and their engagement were coloured by their views of carers not maintaining contact with their relatives, whereas the findings in the next two chapters show that many forensic carers clearly do stay in contact but experience a number of barriers to accessing support. Language or cultural differences were the least cited reasons as to why carers do not use available support. Almost a third of all service respondents gave ‘other’ reasons for carers not using the support provided. These included carers not having time, carers appreciating having less responsibility when their relative was in hospital, previous negative experiences, carers not believing their relative has a mental health problem, or the carer not having a relationship with the patient.
Although the majority (81%) of respondents reported having a confidentiality policy, just three forwarded these to the research team. Three respondents in NHS services did not know if the service had a confidentiality policy.