Historical perspective
The following section discusses the second finding of the empirical analysis. Specifically, it considers enablement first from a historical perspective and then identifies how that has impacted on the arrangements that exist currently.
Analysis of LA committee papers and findings from the interviews confirm that in 2009/10, LA established an enablement service based on a model of operation prevalent throughout Scotland at that time. The teams were introduced to deliver the principles and expectations of enablement across the geographic boundaries and LA was able to establish dedicated enablement by restructured services and re-configuring a hospital discharge team and a crisis care team. As part of the original set up arrangements, therapy services were assigned to the team and played a critical role in determining goal and attainments for individuals. LA’s Occupational Therapists were involved in the establishment and delivery of training events for the social care staff transferring into the new service thereby ensuring that the ethos of enablement was firmly embedded. The close engagement with colleagues from the therapy services at that time was essential in the start-up phase, as well as providing the support and training for front line staff. As one SCO 2 commented in an interview:
Without the help from our colleagues (in the therapy services) we would have been struggling to get off the ground. It wasn’t that we didn’t know what we were doing but they were brilliant at keeping us right without being too overpowering. Their expertise was invaluable as we developed care plans around the service users’ functioning. XX helped me initially to make sure that I was doing what I was supposed to do.
The interviews describe how an eligibility criteria was set against which individuals were selected or de-selected depending on their suitability for an enablement intervention. This criteria was developed to target specific individuals who would benefit from an intensive period of enablement thus leading to better outcomes.
However, a change to the eligibility criteria was effected in 2011 and, as a result of that decision; the enablement service no longer operates on a target specific basis but operates as an initial intake team [The intake approach suggests that all referrals should progress through the enablement team] for the home care service. Consequently, all individuals referred to the LA (except those in the end stages of an illness or with significant cognitive difficulties) are expected to have a period of enablement to optimise their level of functioning and independence. This approach is widely adopted across Scotland (JIT, 2013) on the premise that everyone can benefit from a period of enablement thereby maximising independence and lessening the dependence on services. The decision to switch to an intake model has not been universally welcomed and as one SCO 6 put it:
the intake model creates difficulties
The interviews suggested that the need to change the eligibility criteria was the result of pressures felt across the health and social care sector in 2010/11. At that time, it was reported that there were significant increases in delayed discharges from hospital for individuals in LA (ISD, 2013). From the interviews and from anecdotal information, the general perception was that the length of time taken to undertake an assessment, as part of the discharge protocol, was taking too long. Consequently, key targets measuring the performance of health services were not being met. Therefore, a decision was taken in 2011 to relax the eligibility criteria to the enablement service which had a resultant effect on the Delayed Discharges in LA hospitals. Figure 8 evidences the trend in delayed discharges from 2009 – 2012.
Figure 8 Delayed Discharge (Aggregated) 2009 – 2012. Source: ISD Delayed Discharge
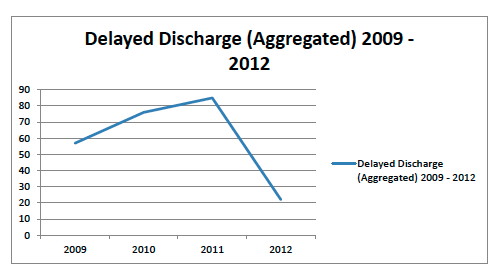
The figure clearly demonstrates that there are now fewer individuals who are delayed in hospitals in LA and that a peak was reached in 2011. By resolving this problem, however, the failure to recognise the cause and effect20 implications have simply shifted the problem across to another part of the system (in this case the enablement teams) but the consequences here are potentially far more reaching. The impact that these decisions have had on the current enablement service are described in the following section. 20 The relation between an event and a second event where it is acknowledged that the first event has caused the second to occur.
Current arrangements
Although the decision to decrease the delayed discharges from hospital increased the number of individuals requiring social care services in LA, no changes were implemented to the staffing levels or the management arrangements of the enablement service to accommodate the change in approach. Alternatively, team capacity that existed at that time was used to absorb the influx of service users. Operationally, the impact on the service has been quite marked and, in particular, the time set aside within the service to develop, implement and monitor enablement programmes of activity has been lost. As SCO 2 remarked:
We have become so inundated with service users who shouldn’t be on our service, we no longer have the time or capacity to deal with enablement
This was further emphasised by SCO4 who suggested that:
The enablement teams are simply chocked up with people…too many people. Previously, we wouldn’t be dealing with many of these people as they would have been deselected
Perhaps the most telling remark was from SCO6:
Enablement no longer works. I’m dealing with people who are in the end stages of their lives and the potential to enable does not exist. The staff has no time any longer to spend with people
These comments in isolation tell part of the story. However, when they are added to the quantitative data, the full impact of the operational shift in approach becomes more apparent. Figure 9 provides a graph of the outcomes for individuals in LA in 2013 following a period of enablement intervention. This graph illustrates three emerging consequences: (i) the number of individuals needing no further (or decreased) service post enablement; (ii) the length of time spent with enablement, and; (iii) individuals returning to hospital during enablement. A further factor was identified by the interviewees in relation to the assessment of enablement users. These are discussed in more detail in the following pages.
Figure 9 Enablement Service Outcomes 2013 Source: LAHCS
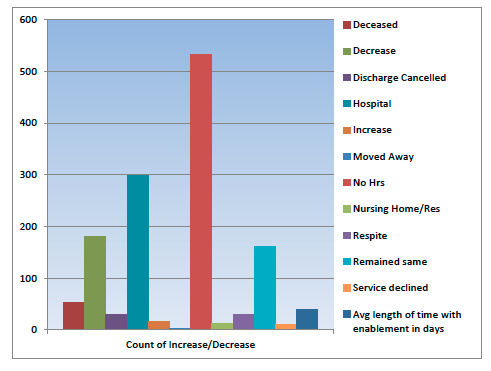
No services required post enablement
The largest peak in Figure 9 shows that over 500 individuals left the enablement service with no hours (or reduced hours) required; this may be considered a positive outcome. Indeed, when this outcome is considered against Figure 6 it could be argued that the small reduction (3%) in total hours committed by LA from 2009 – 2012 may be attributable to the enablement interventions starting to take effect. However, upon closer analysis there is a worrying trend emerging from the data.
Figure 10 percent of service users requiring no (or decreased) hours following enablement. Source LAHCS

Figure 10 shows that in 2010 60% of service users exited the enablement team requiring no further (or decreased) service; by 2013 this had reduced to 42%. This decrease is quite marked and demonstrates a worrying trend because the aim for enablement is to increase the number of service users needing less care, consequently reducing the demand for services in the future. Figure 10 illustrates that there are now fewer individuals exiting the enablement service requiring little or no on-going support than at start-up. Consequently, it is argued that should that trend continue in the years ahead, enablement services will have failed to offset the increased demand and this will result in added pressure being applied to the health and social care sector. For the time being the 42% (2013) requiring no further service or decreased hours remains a positive outcome.
The length of time with enablement
Figure 11 Average number of days on enablement LA. Source: LAHCS
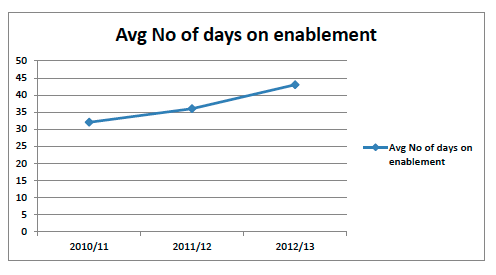
Figure 11 demonstrates that the average number of days that an individual spent on the enablement programme in LA increased from just over 30 days to just over 40 days. The implications of not being able to move an individual on from enablement then mean that there is a reduction in the capacity available within the team which results in fewer people being able to access enablement services. Referring back to the decision to relax criteria to speed up the discharge arrangements from hospital, it is concerning that the capacity needed within the enablement service is being reduced. Social Care Organiser 6 observes:
Six weeks no longer applies in enablement. People remain on the service for as long as needs be now, but it is not to do with the fact that they need further service from us it’s just that there is no place for them to go
The delay in moving an individual on to another part of the service (in-house or external) is commonly referred to as the cliff edge [Term used to describe the feeling of the unknown as people pass from service to service]. Consequently, outcomes for the individual remain uncertain because they don’t know when or which service he/she may be moving on to. Similarly, for the staff charged with the responsibility of managing services or care arrangements, this is equally frustrating as explained:
part of my job is now dealing with frustrated families who are constantly wanting to know whether they can retain the carers that have now or when they are getting new ones.
Social Care Organiser 3
The interviews explained that the longer an individual remains with a provider, then the more dependent they become; when they do eventually move on, then they have to cope with the anxiety of introducing new staff and to familiarise them with individual’s care needs.
Individuals returning to hospital
Finally, an analysis of the evidence also highlighted the increasing number of people who return to hospital following (or during) the period of enablement intervention as being the third factor that inhibits the efficiency of the enablement service. Figure 12 illustrates these increasing numbers over the three years that the enablement team have been operating in LA.
Figure 12 % of individuals returning to hospital during enablement intervention Source: LAHCS
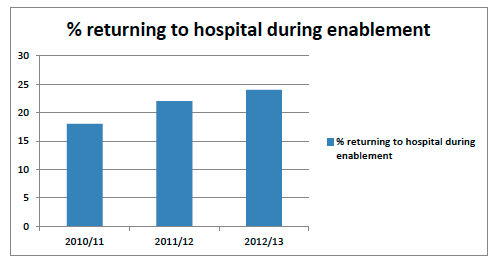
Figure 12 demonstrates that in 2010/11 nearly 17% of people returned to hospital during an enablement period in LA; by 2012/13 this had increased to 24%. The increasing trend is not favourable and the interviews suggested that it places additional strain on the service. They identified two contributing factors: (i) the complex nature of needs that individuals are presenting with, and; (ii) the general frailty of individuals. As SCO 3 confirmed:
we are routinely dealing with people who are very aged. There capabilities are limited and I’m not sure that enablement is right for them.
Figures from LAHCS datasets confirm that the age of individuals who are accepted into the enablement teams ranged from 23 to 99 but that the median age was 83. The predominance of disabilities noted was physical. SCO2 confirmed that the number of people who were presenting as being old-old and very-old [Young-old (65-74); old-old (75 – 84); very old (85+)] was increasing and that their ability to be enabled was severely compromised by their general frailty.
we had someone yesterday who is 99 years old and is pretty much confined to bed…there isn’t much I can do with her other than have her transferred across to the long term services but I know they’ve not got the space so we’ll just need to keep her here until a space is available.
Social Care Organiser 2
Assessment for enablement services
In addition to the three key factors identified in the Figure 10, the interviews suggested that a further contributory factor to the reduced efficiency of enablement was in relation to the assessment for enablement. Assessment for enablement services is carried out by Care Managers [Fully qualified social worker] (CM), either based in the hospitals as part of the hospital discharge service (71%), or as part of the first contact service that receives referrals that are community-based (29%). Several comments were raised in relation to the appropriateness of the assessment received. As SCO 4 claimed:
the assessments that we receive now are not focussed on enablement. Sometimes it seems like it is just a tool to get the person out of hospital
This comment was supported by SCO 8 who suggested that:
the assessment is vital to us to allow us to understand what the person is able to or not do. There have been occasion where I have not known what that is and the person is already home. We’ve then had to rely on our staff going in blind so to speak to review the situation and work out what it is they should be doing.
To date, LA has continued to utilise an assessment framework that is centred on the procedural model [Procedural exists model where the professional gathers information to make a judgement about whether the service user fits the criteria for service provision. . (Harris & White, 2013)] from which a judgement is made on service provision. It is argued that this approach can be a challenge because the emphasis is not on determining the best personal outcome for the individual, but more on whether the individual meets criteria pre-determined by the local authority. In taking forward an outcomes focussed approach – or exchange model [Worker acts as facilitator to generate discussion and assumes that the individual is the best person to understand their needs and outcomes. (Harris & White, 2013) ] – it is vital that outcomes for individuals are the principle driver for activity (Cook and Miller, 2012). Indeed, Miller (2010) argues that implementing personal outcomes approaches such as Talking Points supports organisations to deliver on policy goals, including increased independence, personalisation, enablement, prevention, improved integration and a shift in the balance of care from hospital to the community. Without the proper assessment, then the starting point for a servicer is skewed. If the principles of enablement are not embedded from the outset then there will be operational difficulties experienced throughout the period of intervention. As SCO4 suggests:
assessment is the work book from which we can start the enablement process. If that is lacking in content then we are not able to commence the tasks that we need to start that will help enable the individual. It makes the whole enablement team better than useless