Policy makers in the developed world have been challenged throughout the years to develop strategies that best meet their country’s particular demands for health and social care provision based on their individual demographic patterns. Within a Scottish context, the substantive policy document (All Our Futures: Planning for a Scotland with an ageing population, 2007) sets out a framework that acknowledges the challenges, and seeks to develop an intergenerational, multi-agency approach to tackling the issues. The Communities Minister at the time stated that:
In the context of a changing world and an ageing population, we know that simply relying on our current actions and achievements will not be enough. As we look forward, we will need to ensure that our actions, our services and infrastructure fully reflect and are adapted to our changing demographic picture. Achieving our vision for future generations will not be the result of one strategy or action plan, or the actions of a limited number of people. Each and every one of us will have a role to play if we are to succeed and achieve our aspirations for Scotland’s future.
Rhona Brankin, MSP Minister for Communities, 2007 (p1)
The three primary commitments from this paper for the government of Scotland, and all other stakeholders, were to: (i) work together to develop a shared understanding of the wider implications of an ageing population; (ii) work together to carry through the culture change that Scotland needs, and; (iii) plan effectively for the years ahead (Scottish Government, 2007). In strategic terms, this paper provided the vision for an active ageing population that would continue to contribute to society. To achieve this aim, the Scottish Government set out to establish the opportunities for health, participation and security to enhance the quality of life as people age (World Health Organisation, 2002). Subsequent policy initiatives (Better Health, Better Care, 2007; Health Care Quality Strategy, 2009; Reshaping Care for Older People, 2010) have envisaged an ageing population that will benefit from enabling health and well-being in later life thereby leading to more fulfilling lives (Billiter, 2012). To achieve these outcomes, however, a paradigmatic shift in the way that services are delivered becomes the key factor.
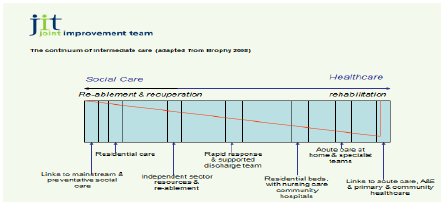
Central to this debate is the role of rehabilitative services and the focus on restorative, recuperative and reconstructive therapies that allow individuals to regain a level of independent functioning (Bowman et al, 1999). Indeed, Foote and Stanners, (2002) describe rehabilitation as the very essence of older people’s care. The Royal College of Nurses (2000) suggest that rehabilitation should focus on re-enablement, facilitating and trying to recapture motivation so as to help people adapt to changes in their life and circumstances. De Monteford University (2007) describe rehabilitation as services for people with poor physical or mental health to help them get better; they define enablement as services for people with poor physical or mental health that cannot help people to get better but helps them to accommodate their illness by learning or re-learning skills necessary for daily living. Brophy (2008) describes rehabilitation as a continuum of intermediate care [Intermediate care is a range of services focussed on prevention, restorative or rehab activity designed to prevent admission to hospital and/or facilitate early discharge from hospital (JIT, 2012)] operating across the health and social care spectrum. Figure 3 provides a schematic. What rehabilitation is and what it can achieve, therefore, proves challenging within the literature. Similarly, extensive debate ensues on the theoretical underpinnings of rehabilitative care. Philips (2005) argues that rehabilitation should remain centred on medical ethics and the doctrine of cure, whereas Young (1996) describes rehabilitation in a more holistic process that factors in the social aspects of community, the personal fulfilment of the individual as well as realisation of full potential. This latter statement is important as it begins to weave the elements (home or homely settings and personal outcomes) that are critical to the development of services that promote active ageing. In either case, however, the development of rehabilitative programmes has played a prominent role both in terms of cost-containment strategies (Office of Science and Technology, 1995), but also to address the changing needs of people as they live longer (World Health Organisation, 1981). In the Delivering Health, Enabling Health policy (2006), the opening remarks introduce the concept of enablement within the context of health professionals such as Nurses, Midwives and Allied Health Professionals (NMAHPs):
Enablement must be the overriding goal of all the services which NMAHPs, and particularly AHPs, offer to their patients…human beings instinctively want to be as self-sufficient and independent as possible and to maximise their physical potential. Patients are their own best carers; you are missing an obvious trick if you do not enable and encourage them to contribute their own ideas and insights and take ownership of their care plan.” Olivia Giles, Meningitis Awareness Campaigner (Delivering Health, Enabling Health Introduction, 2006)
For social care in Scotland, the introduction of enablement is less clear cut. Over time as policy thinking has changed to address the changing demographic or socio-economic circumstances, social care services have evolved from the traditional home help service to introducing community care and delivering personal care services. The establishment of enablement into social care is a continuation of that evolutionary process, but it is one that now represents a crossover into services that have their theoretical underpinnings embedded within the rehabilitative spectrum.
This model suggests that the therapy services can act as the boundary spanner [individuals within organisations who assume the responsibility of spanning operational boundaries and gaining the support of employees (Williams, 2008)] between the elements of social care and rehabilitative care. In particular, occupational therapy skills are central to enablement (Social Care Institute of Excellence, 2011) either for the training and support of social care staff or as integral members of the team. The College of Occupational Therapists (COT) and Association of Directors of Social Services (ADSS) (1995) suggest:
“Occupational therapists within social care services are in a unique position to respond to individual needs through rehabilitation programmes which focus on improving people’s abilities.”
COT:ADSS p3 (1995)
Their importance is further recognised by the need to build effective systems and manage demand by ensuring that the necessary expertise and capacity is available at the point where the service user requires it. The Christie Report (2011) describes this as the need to address the issue of failure demand [Seddon (2007) describes failure demand as increased work caused by the failure to do something right first time for an individual ] within the public services. Seddon (2008) suggests that there is a need to ensure that the right professionals with the right skills are available at the right time to respond to demand. It is through this approach that the right expertise is on-hand to ensure that the work then flows cleanly through the system.
Consequently, it is argued that to embed the enablement ethos it is essential to develop a successful rehabilitative culture within the organisation that harnesses the skills of a range of different disciplines and professionals (Wade, 2004)6. This approach, therefore, considers a multi-disciplinary model that focuses on an individual’s needs and the function of team members. This pooling of resources to achieve better outcomes was a central feature of the development of intermediate care services in England in the early 2000s. The concept of intermediate care was to enhance the independence of older people in an attempt to prevent the admission to hospital and reduce costs and promote better quality of life (DOH, 1997). Within this model, Brophy (2008) describes the various stages of rehabilitation and identifies the individuals who may assume responsibility for the delivery of the service. See Figure 3. 6 The notable exceptions to this organisational ideology are where individuals present in the end stages of an illness/life or where there are significant cognitive challenges.
Figure 3 Brophy’s Continuum of Intermediate Care. Source: Adapted from JIT
In Scotland, a delivery framework for adult rehabilitation (Scottish Government, 2007) was developed that focused on three key groups – older people, adults with long-term conditions and people returning from work absence and/or wishing to stay in employment – and it aimed to maximise individuals’ participation in their communities and improving quality of life for them, their family and carers. Reports such as the Better Health, Better Care (2005) and Reshaping Care for Older People (2010) call for a significant shift in health and social care services in the community to support this overall policy by developing innovative health and social care services. The limited success of these policies and the development of joint initiatives lie in part to the organisational difficulties that extend across the health and social care sector (Griffiths, 1988). The introduction of the legislative programme to integrate health and social care will provide the legal framework for improved, collaborative working in the years ahead (Scottish Government, 2013).
Enablement is a preventative, restorative approach to the delivery of care at home services that has its focus on maximising independence for individuals and getting them to do for themselves rather than have done for them. The literature shows that when introduced properly there is time savings to be made for the providers of care. The important thing here is that the time saving can then be recycled and used with other service users thus allowing the service provider to do more with the same resource. The benefits for the service user are a general satisfaction with increased well-being, health and mood. The introduction of enablement services is viewed as one of the key government-led initiatives that will fulfil policy objectives, promote active ageing, deliver better outcomes for people and offset the increase demand for services in the years ahead. However, no formal policy document exists that establishes enablement within social care in Scotland, more simply an initiative from the Joint Improvement Team [Organisation established in 2004 to offer practical assistance and managerial capacity to health and social care partnerships.] (JIT) to follow the examples of good practice evidenced in England was promoted from which the organisations took their lead (NIHR 2010). JIT has played a central role in facilitating and supporting the introduction of enablement practice in Scotland assisting the local authorities to embed enablement practices and make the connection to relevant national strategy and policies (Intermediate Care Framework; National Dementia Strategy; Talking Points; Self Directed Support; Delayed Discharge; Reshaping Care). From a recent survey of all the Scottish local authorities, the JIT (2013) reported that 78% of the Scottish local authorities now have an enablement service with the remainder in the development stage of such services.
The introduction of enablement as an approach to support individuals at home is a significant initiative and one that aims to address the increased demand for service in the forthcoming years (JIT, 2010). Further, the introduction of such services are seen as a key development in care at home services that can prevent or delay the need for more costly, intensive services but can promote the quality of life of older people by maximising independent living (Anchor, 1996). In 2011, the Institute of Research in Social Services (IRISS) described enablement within the policy context as a means of assisting individuals to lead full and independent lives whilst reducing the overall cost of provision.
At the centre of the redesign programme is the shift from traditional care provision based on task and time [Task and time services refer to dedicated times allocated to frontline staff to carry out specific support tasks to service users.] to one that adopts the principles of enablement at its core. Thus, enablement is designed to help people learn or relearn the skills necessary for daily living which may have been lost through deterioration in health and/or increased support needs. A focus on regaining physical ability is central, as is the active, functional assessment processes at the outset that determines capabilities and establishes what realistic outcomes can be achieved (Francis, et al 2011). By adopting such an approach, programmes of activity are designed to optimise an individual’s level of functioning thus restoring their ability to perform usual activities and, consequently, improve their perceived quality of life. In practical terms, an enablement intervention lasts for a short period of time, usually for a six week period, where the individual and the enablement staff focus on the programme of activity and work towards achieving the personal goals and outcomes instead of simply meeting needs. Consequently, enablement teams need to have trained staff with the appropriate skills and the mind-set to support individuals with their programme of activity. Records of achievement, goals attained and outcomes reached should be made at each contact and the programme of activity adjusted in accordance with changing circumstances (Francis et al, 2011). Above all, however, longer, more responsive and flexible visits are essential to allow the time required to work through a programme of activity and achieve satisfactory outcomes for the individual and the services.
Evaluations of the early adopters of home care enablement (Glendinning and Newbronner, 2008; Mcleod and Mair, 2009) report significant benefits to individuals and health and social care partners although more recent reports (Francis et al, 2011; JIT 2013) begin to raise concerns about the greater costs of enablement compared with conventional home care and the organisational implications of establishing and maintaining an enablement service. Indeed, Francis (2011) suggests that:
enablement requires substantial up-front investment, which is greater than the cost of providing conventional home care. A typical enablement intervention costs around £2000 compared with £1392 for conventional home care over a comparable period
SCIE, Research Briefing, 2011 No 36 p9
What becomes apparent from the literature is that the evidence base around the overall success of enablement services is inconclusive. There is significant writing in descriptive terms around what enablement interventions can potentially achieve and the processes that need to be followed to establish services (Care Services Efficiency Delivery, 2007; Pilkington, 2008; Rabiee, 2009) but less evidence has been produced which would allow policy-makers or researchers to draw definitive conclusions on its overall effectiveness to achieve its outcomes (DEMOS, 2012; Whitehead et al 2013). Further, the majority of the analysis to date has been carried out on English local authorities and the only published work on Scotland relates to the City of Edinburgh (Mcleod, Mair and RPM Associates, 2009) and Glasgow City (Ghatorae, 2013).
Despite an extensive search of the literature, none could be found that considers the direct impact of the ageing population on social care services today using a case study methodology. Searches of the Health Management Online and the Social Services Knowledge Network databases only produced a small number of reports that were relevant. This dissertation, therefore, attempts to address this gap in literature through a mixed methods study carried out in one case study site that sought to answer the following research questions:
- What is the demographic context in which social care services are being delivered today.
- What is the approach taken to enablement in LA.
- To what extent are enablement services offsetting and preventing increased service demands.
- What are the factors that are impacting (positively or negatively) on LA ability to deliver enablement services.
- Finally, what are the recommendations for future policy and practice in the years ahead.